Improving Early Thermal Care for Preterm Infants
Joint maternal-neonatal safety collaborative projects to increase the number of preterm neonates admitted on to a neonatal unit with an admission temperature between 36.5°C to 37.5°C.
Case example – Oxford University Hospitals NHS Foundation Trust
The Initial Problem and its Impact
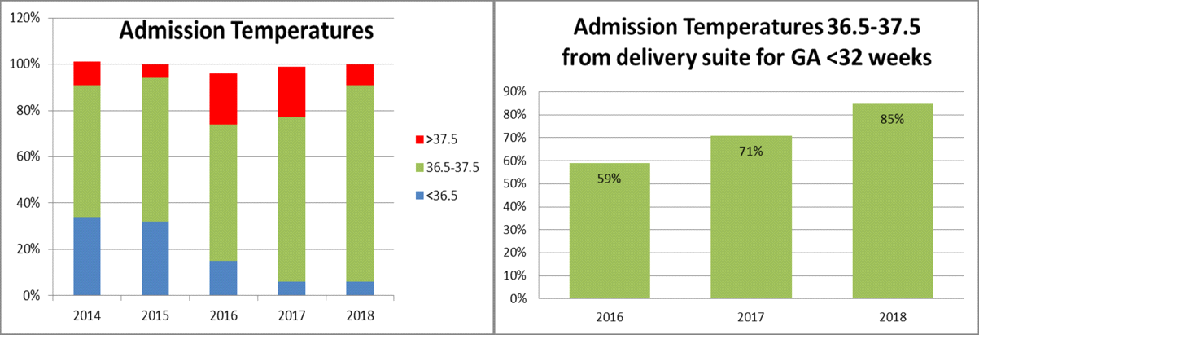
Normothermia on admission for infants born at less than 32 weeks gestation as measured by the National Neonatal Audit Programme had remained static at around the national average between 2014 and 2016 (57% in 2014, 62% in 2015, and 59% in 2016). Therefore, we initiated a quality improvement project to address this in January 2017 and adopted this as a joint maternal-neonatal safety collaborative project from November 2017 onwards.
Causes of the Problem
- BadgerNet data was reviewed, looking at temperature on admission for different gestational ages and weights, whether babies were too hot or too cold and where they were admitted from (theatres etc).
- Four stages were identified from birth to neonatal unit admission where temperature management could be compromised (Figure 1).
Figure 1: The thermal care journey.
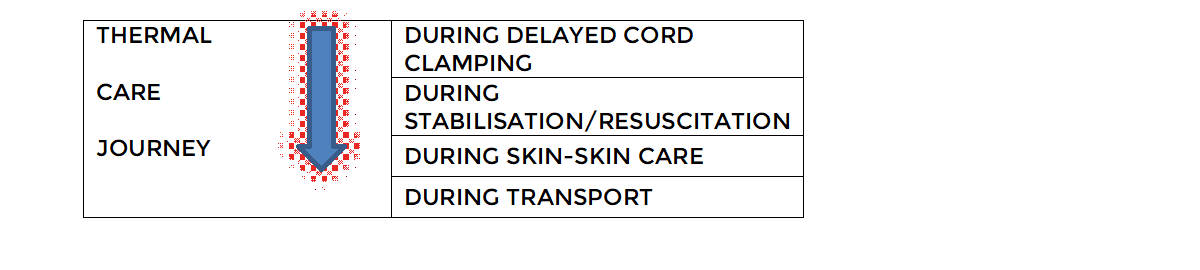
- Thermal care guidance was issued covering each stage of the journey from birth to neonatal unit admission.
- A standardised case review template was used for any case where temperatures were outside the normal range.
- Monthly feedback to staff via newsletters and posters.
Project Aim Statement
By end of December 2018, 90% of preterm neonates of less than 32 weeks gestation born in the delivery suite would have a neonatal unit admission temperature 36.5°C to 37.5°C.
Stakeholders
The key stakeholders for this project were neonatal unit medical and nursing staff, midwifery and obstetric staff (particularly delivery suite and theatre staff).
PDSA Cycles / Solution(s) Tested
- A new thermal care guideline including measurement of temperature in delivery suite and use of servo-control temperature for infants <32 weeks (February 2017).
- Preterm infant resuscitation thermal care training (March 2017).
- All hat sizes readily available on resuscitaires (November 2017).
- Room thermometers in highest risk delivery suite rooms (Dec 2017).
- Simulation of use of an incubator shuttle for transfer from delivery suite to the Neonatal Intensive Care Unit (Jan 2018) – rejected. Continue with transfer on resuscitaire.
- Sterile plastic bags (NeoHelp, Vygon) introduced for caesarean sections (Feb 2018).
- Reduced use of transwarmers as overheating (Feb 2018).
- Improving access to skin probes for servo-control on resuscitaires (Feb 2018).
- Thermal care ‘grab bags’ for delivery suite. Consists of: hat, skin temperature probe, plastic bag, small face mask, and scissors (March 2018).
- Education – ‘Big 5’ poster recirculation (July 2018).
- Education of new staff members (September and January 2018).
- ‘How to use Servo mode’ temperature guide added (January 2019).
Data Results
Figure 2: Administration temperatures over time.
How This Improvement Will Be Sustained
- Measure temperature in delivery suite and on arrival in neonatal unit.
- Servo-control temperature for babies less than 32 weeks gestation (training required) (Figure 3).
Figure 3: Servo-control temperature.

- Dry the head and use an appropriately sized hat.
- Use of plastic bags whilst delaying cord clamping (sterile for C-section).
- Thermal care grab bags are useful to ensure you have all the kit available.
- Avoid overuse of transwarmer.
- Regular staff training.
- Monthly feedback.
Challenges and Learnings
Perseverance with messages and training were key to overcoming barriers as well as regular feedback to staff on our improvements.
This project improved working relationships between obstetric/ midwifery/ theatre and neonatal staff.
Suggestions For Further Implementation
- Have clear goals.
- Make sure the required kit is always easily accessible and everyone knows how to use it.
- Involve midwives and obstetricians.
- Regular multidisciplinary meeting to review previous goals and to set new ones.
- Regular education and feedback to neonatal and maternity team on how we are doing.
Project Lead: A Bowring (ANNP), J Yong (ST7), A Williams (QI Midwife), H Threlfall (Midwife, Delivery Suite Manager), K Lean (Patient Safety Manager, Oxford AHSN), E Adams (Consultant Neonatologist)
Organisation: Oxford University Hospitals NHS Foundation Trust
Published: February 2020
Case example – South Tees Hospitals NHS Foundation Trust
Background
Admission temperature is a very strong and important predictor of neonatal mortality and morbidity especially in preterm neonates in a number of studies. Hence it is considered an important healthcare quality indicator in the NICU. Hypothermia is associated with adverse pulmonary symptoms (increased need of respiratory support) and other serious preterm morbidities e.g. intraventricular haemorrhage, bronchopulmonary dysplasia, necrotising enterocolitis, retinopathy of prematurity and late onset sepsis in observation studies.
We had high admission hypothermia rates – our rate of normothermia was 50%, compared to network and national average of 65% and 71% respectively. This cannot be explained by one single factor. Hence there was an urgent need to understand the reasons for temperature loss by starting a quality improvement initiative. Thermo-regulation In Preterm neonates (TRIP) project was started to improve admission normothermia in preterm neonates < 32 weeks.
It was evident that there is a clear lack of leadership in taking responsibility for thermoregulation with major focus of the team on the airway, breathing and circulation.
The windows of the delivery suites and the doors of theatre were being kept open with poor awareness of optimal temperature range amongst midwives and the parents. Also, there was no room thermometer in the delivery rooms which left the temperature assessment very subjective.
There were equipment issues e.g. there was a clear difference in the displayed temperature and the actual temperature in the transport trolley with lots of ‘holes’ in the insulation.
Furthermore, there was no departmental policy regarding the thermal care during delayed cord clamping which was again not helping with maintaining a warm chain of temperature.
Projects aims
- To decrease any admission hypothermia (defined as < 36.5 C) in < 32 weeks gestation preterm neonates by 10-20% in 6-12 months.
- To decrease any admission temperature <36 C in < 32 weeks infants by 10-20% in 6-12 months
- To improve rates of normothermia in preterm infants <32 weeks by 10-20% in 6-12 months.
Project stakeholders included; nursing staff, ANNPs, trainees, midwifery staff, consultants & managers
Measures
- Admission normothermia rate as percentage
- Admission Hypothermia rate as percentage
- Number of checklist/Audit forms completed in eligible babies
- Completed temperature readings at key stages in eligible babies
- DATIX completed in eligible neonates
Our improvement plan
Introduction of checklist with multiple temperature checks – the checklist acted as a prompt to the staff to prepare the environment and the equipment. This also acted as a data collection form and a tool to understand the key stages where the temperature is lost and then targeting out the interventions in the long term.
The five temperature checks were:
- Just after stabilisation (T1)
- Before leaving the resuscitaire (T2)
- Before setting off in the transport shuttle (T3)
- After reaching the NICU in the shuttle (T4)
- In the cot in NICU (T5)
Pre-brief /Huddle before delivery – a brief pre–delivery huddle to allocate roles and responsibilities.
Thermoregulation role to a specified member of the team – by default it was allocated to the nursing staff but helping with it was everyone’s responsibility.
Poster for delivery room windows – helped with increasing the awareness among parents and midwifery staff about not unnecessarily opening the windows.
Thermometer in the delivery rooms – for objective awareness about delivery room temperature. The delivery room/theatre temperature was recorded on the checklist. Also, a portable battery-operated room thermometer was used by team in case of nonworking/missing room thermometer.
Datix reporting of admission hypothermia of <36.0 C – all cases of admission hypothermia < 36.0 C were reported on the DATIX system. They were followed up by the TRIP team to identify any new learning.
Replacement of the old transport shuttle with new one – the old transport shuttle was replaced with a new one. Humidification of gases were not done because of logistic issues. Multiple session of training and simulation were done with the staff with the new shuttle.
Replacement of plastic wrap with the new sterile plastic bags – these sterile plastic bags were introduced with advantages of complete sealing of the body apart from the face.
The biggest barrier was team buy-in. It was approached by motivating and involving everyone in the project, presenting improvement in hypothermia data and key learning points in a monthly newsletter.
Another major concern was adding to the workload to the already busy nursing staff during delivery. So, the job of temperature checks was shared between medical, nursing and midwifery teams.
Procurement of the new plastic bags was another challenge. The company representative was contacted for free samples. The unit consultant with previous experience with these bags undertook teaching and training of the staff. The new bag was procured by regular purchase after approval in consultant meeting.
Outcomes
The 2019 NNAP data published in 2020 showed that admission temperatures in preterm infants <32 weeks were around 50% in normothermia range at JCUH. Around 21.5% of infants had moderate hypothermia, <36 C.
Within 6 months of the introduction of the initiative (see Figure 4):
- Around 63.5 % of infants have remained in normothermia range (36.5-37.7 C)
- The rates of admission temperature <36 C have been reduced from 21.5 % to 6.3%
- The rates of admission hypothermia <36.5 C have reduced from 32.5% to 14.3%
Figure 4: Normothermia and hypothermia before and after introduction of QI bundles.

Challenges and learnings
Checklists initially showed an average drop of 0.5 C between T3 and T6, so infants were kept on resuscitaire until the axillary temperature is at least 37 C before moving to transport shuttle.
Delivery room and theatre resuscitaires were changed (not as part of project) during the project. The new resuscitaire have more efficient heater output which resulted in an increased number of hyperthermic neonates. Although our normothermia rates reduced drastically, normothermia rates were offset by rise in number of hyperthermia.
There was frequent staff change (new MTI doctors, new nurses, rotation of the trainees) during the project which puts a challenge on keeping up with the training on the project.
As with any other QI project, the motivation of the staff decreases after first few months, so it is really important to keep them motivated by giving shout outs and frequent reminders. The key to success is persistence. There will be moments of disappointment, challenges and feeling of failure.
Top tips for implementation
Combining multiple interventions to avoid heat loss, together with the use of checklists and continuous feedback to the staff, are universally applicable in maintaining normothermia.
Local simulations and hypothermia case reviews will give important information about the key local problem areas to target in the QI.
Rather than individual efforts, forming an MDT QI team of people who are passionate for temperature control is the most important step to achieve success.
Authors: Vrinda Nair (Consultant Lead), Anip Garg (Trainee Registrar Lead), Sian Oldham (ANNP Lead), Zoe Musgrave & Emily Stalker (Nursing Lead), Elizabeth Schonewald & Lisa Foster (Nurse Educators)
Organisation: South Tees Hospitals NHS Foundation Trust, James Cook University Hospital, Middlesbrough
First published on QI Central in July 2022