Reducing Necrotising Enterocolitis: A Quality Improvement Initiative
Raising awareness of the risk factors linked to necrotising enterocolitis to decrease its incidence on a neonatal unit at West Hertfordshire NHS Trust.
The Initial Problem and its Impact
Necrotising enterocolitis (NEC) is a neonatal emergency mainly seen in preterm infants. It can have devastating consequences including delayed feeding, surgery, short gut, poor growth, increased hospital stays, delayed neurodevelopment and death. In the UK, 1 in 20 preterm infants born at less than 32 weeks gestation are at risk of NEC with high mortality rates of more than 20%.
Causes of the Problem
In 2017, the neonatal unit at Watford General Hospital stood out as having a high rate of NEC compared to units of the same level, our network and nationally (Table 1).
Table 1: NEC results from National Neonatal Audit Programme 2018 report (2017 data)

Project Aim Statement
The study aim was to understand the risk factors linked to NEC and decrease the incidence of NEC at our unit by 50% within one year using structured quality improvement (QI) methodology.
Stakeholders
All key stakeholders were engaged (including parents) in the discussions. In particular, we would like to acknowledge Bhavani Sivakumar, Neonatal Data Administrator and the neonatal team, external reviewers, parents and families for their participation and engagement in this collaborative quality improvement initiative.
PDSA Cycles / Solution(s) Tested
- External thematic review was sought in view of the high incidence of NEC.
- Modifiable contributing/causative factors and themes were identified.
- Extrinsic risk factors such as enteral feeding practices, compliance with network NEC bundle, relevant medication exposure (ibuprofen, anti-reflux medication), blood transfusion and sepsis were investigated.
- Appropriate QI tools were used to drive changes to decrease the NEC rate (Figure 1).
- Process changes were monitored by iterative plan, do, study, act (PDSA) cycles and NEC occurrences were tracked using statistical process control (SPC) charts – ‘days between NEC’ for the next 12 months.
Figure 1: Driver diagram to inform change in ideas.

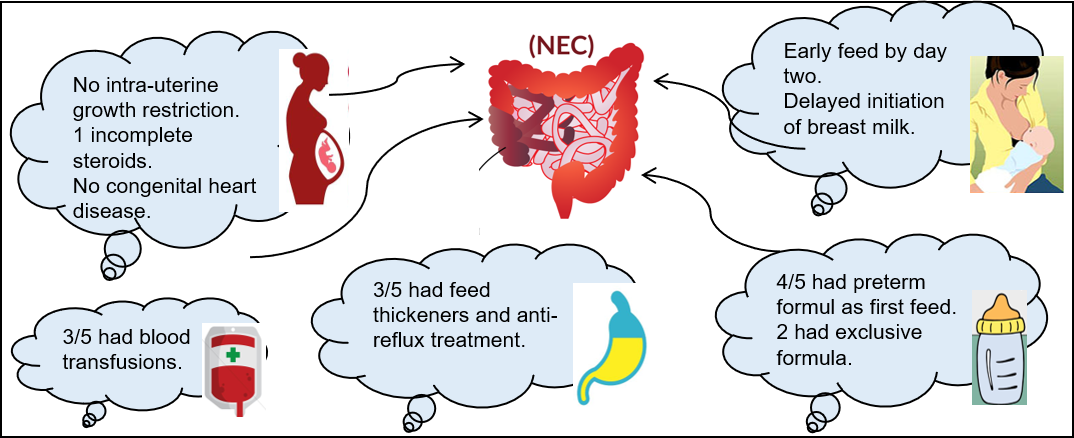
- A pareto chart identified key risk factors for NEC and raised awareness of key issues (i.e. early initiation of formula feeds when mother’s own milk was not available, anti-reflux medication and blood transfusion).
- Awareness was raised about NEC related complications (Figure 2): antibiotic duration, prolonged parenteral nutrition, surgery, delayed discharge and poorer developmental outcome.
Figure 2: Factors related to NEC.
Data Results
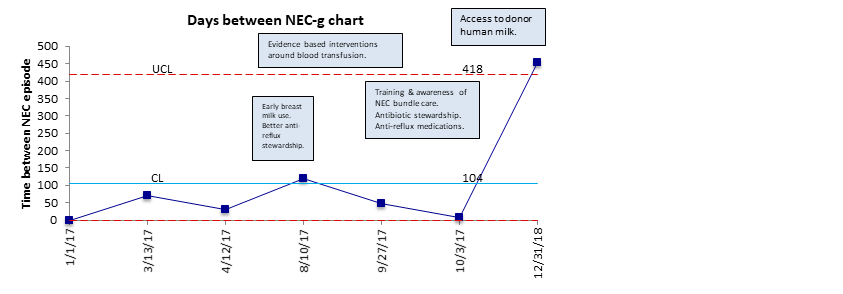
- Following QI initiatives in 2018, 0 of 29 eligible babies had NEC.
- The average number of NEC-free days increased from 55 to 350. The average number of patients between NEC events increased from 4 to 32 (Figure 3).
Figure 3: Days between NEC-g chart.
How This Improvement Will Be Sustained
Use statistical process control tools for real-time monitoring of adverse events.
Challenges and Learnings
Engage all key stakeholders including parents when discussing NNAP report findings.
Suggestions for Further Implementation
Scale-up and spread findings to the wider neonatal community.
Project Lead: S Narayanan, C Dawson, N Merchant, Department of Neonatology & Paediatrics
Organisation: West Hertfordshire NHS Trust, Watford, UK
Published: February 2020