Multidisciplinary Team Working to Standardise Neurodevelopmental Follow-Up
Two case examples of multidisciplinary approaches to using QI methodology to improve the delivery, uptake and recording of two-year developmental assessments for children born preterm.
Royal Hospital for Children, Glasgow
Our neurodevelopmental outpatient service has undergone redesign with reference to recently published NICE Guideline (NG 72) ‘Developmental Follow up of Children and Young People Born Preterm’ in August 2017 and Scottish Government neonatal care strategic plans in ‘The Best Start: Five-year Plan for Maternity and Neonatal Care’ in January 2017.
Causes of the Problem
Prior to the 2017 publications from NICE and the Scottish Government, we did not use a standardised assessment at two years corrected age and did not regularly report two-year outcome data.
Project Aim Statement
To use QI methodology to improve the delivery, uptake and recording of our two-year developmental assessments.
Stakeholders
The project team, comprised of professionals from neonatology, physiotherapy, speech and language therapy and neonatal liaison, met quarterly to review and refine our plan. In addition, we held a national meeting with neurodevelopmental teams from across Scotland to share knowledge and experience within varied clinic settings.
PDSA Cycles / Solution(s) Tested
Our improvement project is summarised in the driver diagram (Figure 1).
Figure 1: Driver diagram, neurodevelopmental follow-up improvement project.

Data Results
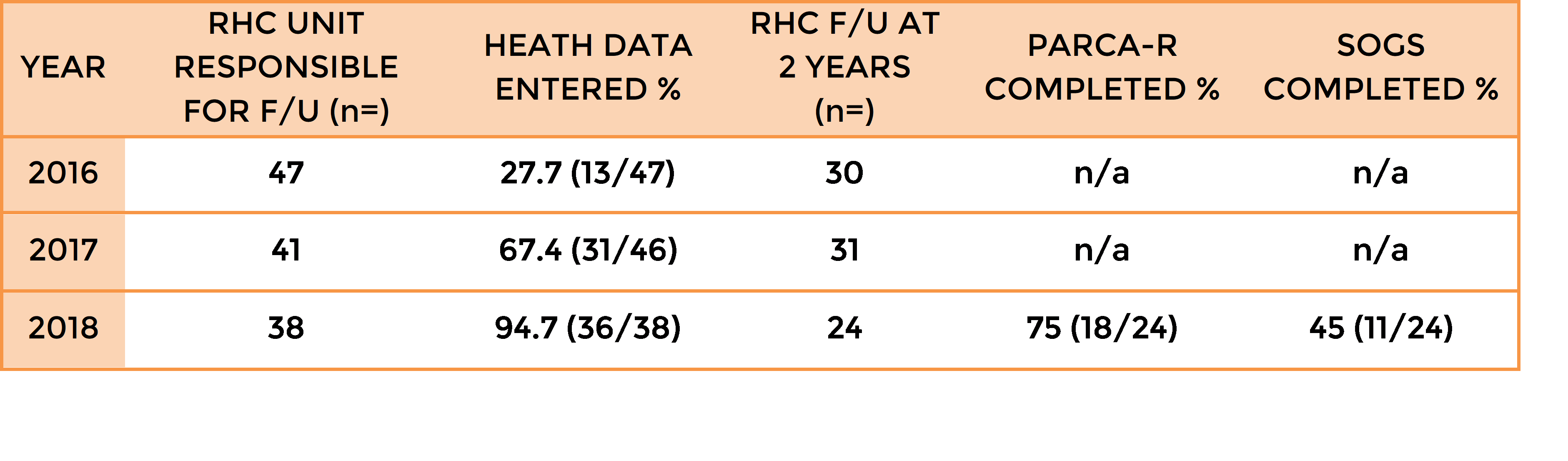
We have increased the number of two-year outcomes reported to NNAP, with over 94% of children in 2018 with health data entered (Table 1). Through collaborative working with neonatal units across Scotland we achieved high rates of follow-up reporting for children who had been discharged home from our neonatal unit that we had previously considered ‘responsibility of another unit’.
The Parent Report of Children’s Abilities Revised (PARCA-R) questionnaire and Schedule of Growing Skills II was introduced to our clinic during the 2018 data collection year which accounts for those children with incomplete assessments (12 and 6 children had been discharged prior to the introduction of SOGS and PARCA-R respectively). Since its introduction, 100% of families attending RHC clinic at two years corrected, have completed a PARCA-R questionnaire.
Table 1: NNAP follow-up and completion of standardised 2-year assessment rates.
How This Improvement Will Be Sustained
We have established a safe, equitable, efficient and cost-effective service that offers families a one stop clinic, delivered by a skilled multidisciplinary team.
Hear from a family who attended our clinic:

Challenges and Learnings
Top tips for implementation:
- Establish a core group of invested multidisciplinary professionals to deliver neurodevelopmental follow-up for your unit.
- Engage with families to provide feedback on and improve your neurodevelopmental follow-up service.
- Collaborate with other units in your network to achieve consistently high follow-up rates.
- Review your data throughout the year. If it is not what you anticipated, look more closely at the quality and accuracy of data input.
Suggestions For Further Implementation
We will continue to aim to empower parents, recognising they play an integral role in their child achieving their developmental potential.
Project Lead: Dr Louise Leven, Consultant Neonatologist, Alison Grant, Physiotherapy Service Lead, Sara Russell, Speech and Language Therapy Clinical Lead
Organisation: Royal Hospital for Children, Glasgow
First published in the NNAP Annual Report 2020
Watford General Hospital, West Hertfordshire NHS Trust
Background
Woodland Neonatal Unit at Watford General Hospital, West Hertfordshire NHS Trust caters for up to 1200 admissions per year. It is one of the busiest level 2 units within the East of England Neonatal Network. The unit has contributed data to the NNAP since its inception in 2007. Completion of 2-year outcome assessment forms for babies born less than 30 weeks gestation was less than satisfactory (≤ 80%) in 2013/2014. Moreover, none of this cohort of babies had a formal neurodevelopmental assessment.
In this case study, we demonstrate how we have used NNAP 2 year follow up data benchmarks to guide our quality improvement project. We show how we improved data completion rates while at the same time increasing the proportion of babies who had a formal developmental assessment.
What we did
We arranged for brainstorming sessions between all relevant stakeholders to identify key areas for improvement and discussed potential solutions:

A specialist clinic was set up to improve compliance:
- The team included a neonatologist, physiotherapist and a clinic coordinator.
- Eligible infants born at <30 weeks were prioritised.
- Appointments were given on discharge and reminders & alerts were set up for 18-30 months range.
- Bayley Scales of Infant & Toddler Development III (BSID) were used for the assessments.
- A BadgerNet data analyst was appointed to facilitate real time data monitoring which allowed zero latency feedback to the lead consultant.
What we achieved
The table below shows steady improvement from 2013 to 2017 in the results for the NNAP audit measure of 2-year health status follow-up completion. There was a small decline in 2016 as 2 babies were seen outside the 18-30 months’ target. BSID assessments increased from 0 in 2013 to 94 % in 2017. ‘Did Not Attend’ rates increased initially in 2015 on introduction of the Bayley Assessment Clinic but using iterative PDSA cycles, this was brought down to 6% in 2017:
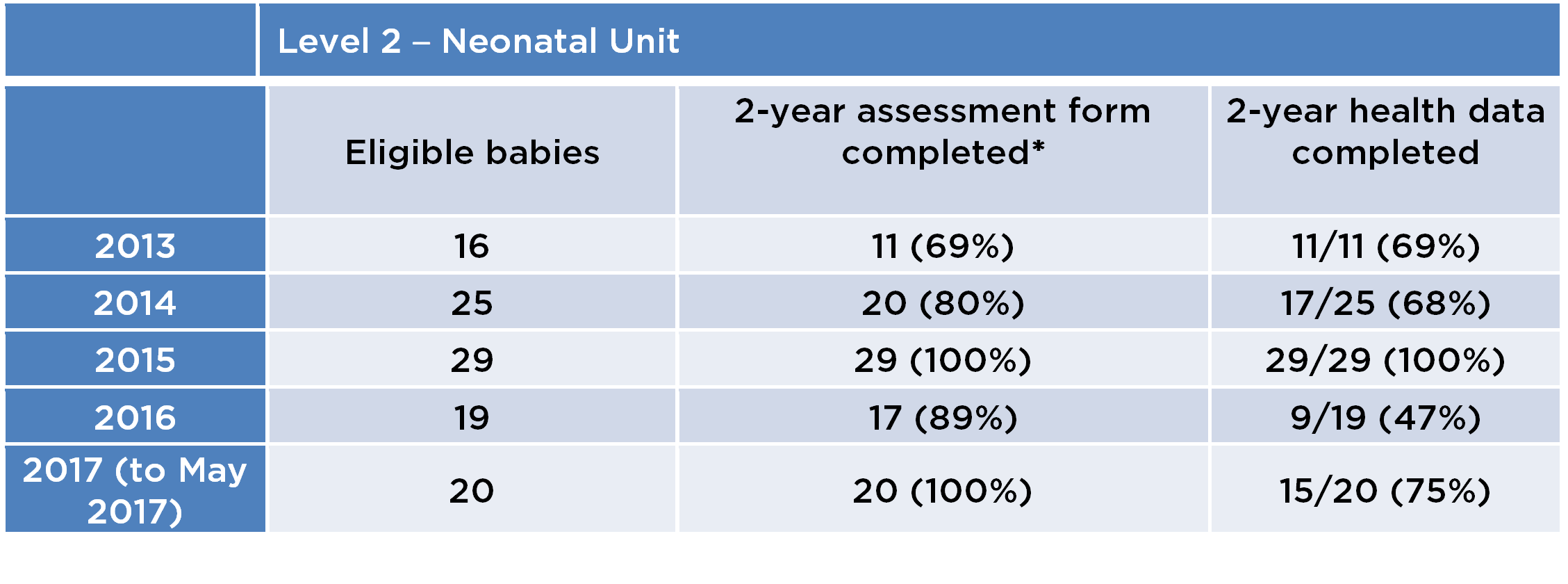
*(The results in this column include babies for whom any data was entered, not only health data i.e. “Not assessed for other reason” and “Lost to follow up”
Parental feedback was obtained through an anonymous questionnaire at the end of each clinic appointment which asked about pre-clinic communication, in clinic experience, parent understanding of process and communication of BSID outcomes; parents rated the service as ‘very good’ (5.5/6 on Likert scale).
Suggestions for adaptation for other units
- Engage all key stakeholders when discussing NNAP report findings
- Dedicate resources towards clinic administration/data entry and feedback
- Multidisciplinary set up ideal for Bayley clinics
- Active clinic management to reduce DNA rates
- Set up avenues for user (parent) feedback
- Patients who move out of area pose a unique challenge for completion of 2 year outcome assessments and influence outcome data. We would also suggest that NNAP/BadgerNet develop mechanisms to allow reassignment of patients to units closer to their home.
Authors: Dr Sankara Narayanan (Consultant Neonatologist & NNAP lead), Dr Nazakat Merchant (Consultant Neonatologist & Lead for High Risk Neonatal Follow-up Programme), Sarah Beasley (Paediatric Physiotherapist), Bhavani Sivakumar (Badgernet data analyst), and Pauline Southernwood (Clinic coordinator)
Organisation: Watford General Hospital, West Hertfordshire NHS Trust
First published in the NNAP Annual Report 2017