Using Quality Improvement Methodology to Reduce Central Line Associated Blood Stream Infections
Reducing harm from Central Line Associated Blood Stream Infection as part of the Scottish Patient Safety Programme and Maternal & Children’s Quality Improvement Collaborative.
Background
The neonatal unit of the Royal Hospital for Children in Glasgow was formed in 2015 by the merger of the Royal Hospital for Sick Children (Yorkhill) and the Southern General Hospital (SGH) neonatal units on the site of the latter. It consists of 50 beds and provides tertiary level care including surgery, neurosurgery and all neonatal cardiac and ECMO services for Scotland. The unit is part of the West of Scotland Managed Clinical Network and has been contributing to National Neonatal Audit Programme (NNAP) data since 2015.
Processes that were in place before 2016
Since 2013 the unit has participated in the Scottish Patient Safety programme. The Maternal & Children’s Quality Improvement Collaborative (MCQIC) arm of the programme has supported units in using quality improvement methodology to reduce harm. This has included education in QI methods, sharing of practices between Scottish neonatal units, advice from Improvement Advisors as well as provision of a spreadsheet toolkit for data collection and analysis. We worked with the programme to reduce harm from Central Line Associated Blood Stream Infection amongst several other strands of work.
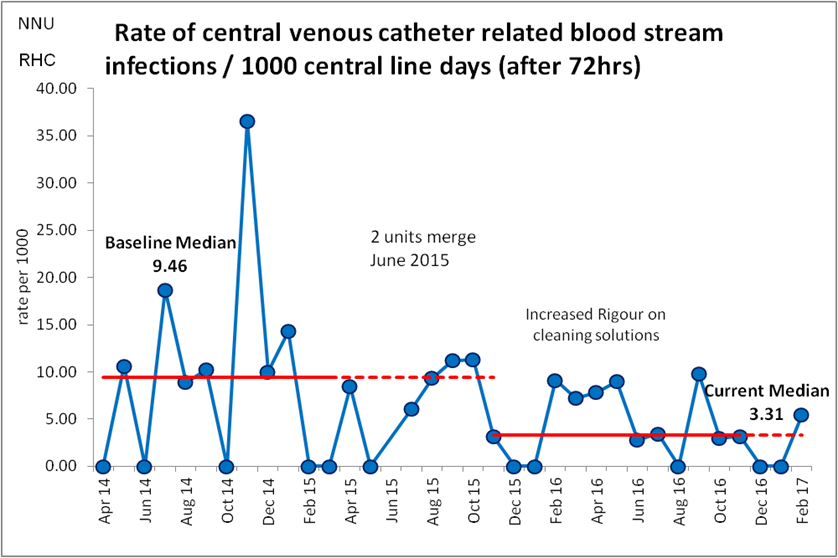
When data was first collected in April 2014 on the SGH site, there was an average of 101 line days per month. The median CLABSI rate per month was 9.46 per 1000 line days over the first 12 months during which testing improvements was ongoing. This is based on the NNAP measure of proportion of babies with positive blood culture after 72 hours of age when central line present, standardised to a rate per 1000 catheter days. After merging units the number of line days increased to 409 per month.
What we did
Standardising Process
Central Line insertion and maintenance bundles were used to standardise processes.
Key elements of insertion included:
- Two person technique
- Use of hat, mask
- Gown & gloves,
- Use of appropriate cleaning solution,
- Securing with a standard technique and documentation of line tip position.
An auditable checklist was developed for the assistant and a sticker developed for documentation. These were used for both umbilical and percutaneous (PICC) catheters. Lines inserted in theatre did not use an insertion checklist.
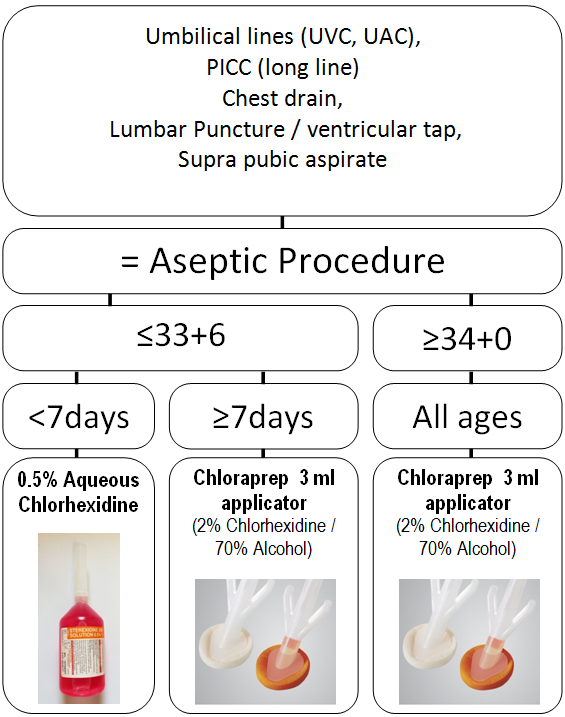
Early testing indicated the need for clarity around cleaning solution. Agreement was reached between clinicians and the local Infection Prevention Team to use 0.5% Chlorhexidine for babies born <34 weeks in the first 7 days of life. In all other circumstances 2% Chlorhexidine in 70% alcohol would be used. Using multiple Plan, Do, Study, Act (PDSA) cycles, an A4 poster was developed and placed around the unit:
Key elements of the maintenance bundle included daily review of the need to keep the line in situ, the use of needle free adaptors on all ports which were changed every 3 days, dressing change unless clean and secure and appropriate hygiene before accessing the port. The latter currently consists of hand washing and the use of sterile gloves.
Tests of Change
Whilst compliance with insertion and maintenance bundles appeared to be relatively good there was no improvement in CLABSI rates. In response to this, the combined checklist and audit forms were considered in detail in May 2016. This revealed that the checkbox relating to the “appropriate cleaning solution” was often given a positive response by the assistant but in effect the lower strength cleaning solution was being used in cases where 2% chlorhexidine and alcohol was expected. This afforded an opportunity for further tests of change.
An updated education package was developed for new registrars with some success but it is well recognised that education of the current workforce, especially when many only work in the neonatal unit for six months, will not necessarily lead to long term sustained improvement.
A physical change was required and as such all cleaning solutions of 0.5% Chlorhexidine were labelled with details of babies in whom it’s use is appropriate and the word “WEAK” in bold. This design was settled upon after testing different options. We then saw our compliance with the process measure of appropriate skin cleansing increase to 88% from 44%:

Overall compliance shown in the run chart below represents the percentage of babies in who all elements of the bundle were complied with:
Alongside work on insertion, the nursing team focused on the regular changing of smart sites, promoting asepsis when accessing lines and ward round review of the need for central access, aiming to remove lines when babies reach 120ml/kg/day of enteral feeds where there are no complicating factors eg surgery.
What we achieved
Sustained Improvement
From November 2015 there has been sustained improvement, with 13 consecutive months on or below the baseline median of 9.46. The new baseline of 3.31 CLABSI per 1000 line days per month represents a 65% reduction in the median. Work is ongoing to further reduce this rate with the introduction of a new SPSP Central Line bundle in May 2016.

Acknowledgements
Dr Dhulipala Anand was instrumental in introducing the original central line bundle in RHSC (Yorkhill), Dr Sumaiya Cassim diligently analysed audit forms and Senior Nurse Natalie Houston has led the improvements in central line maintenance. Their time and efforts are much appreciated.
Project Lead: Dr Colin Peters, Consultant Neonatologist
Organisation: Royal Hospital for Children, Glasgow
First published in the NNAP Annual Report 2017